The National Pressure Ulcer Advisory Panel (NPUAP) serves as the authoritative voice for improved patient outcomes in pressure injury prevention and treatment through public policy, education, and research. The objective of STOP logo 2017 World Wide Pressure Injury Prevention Day is to increase national awareness for pressure injury prevention and to educate the public on this topic. NPUAP has developed an extensive media materials package appropriate for all healthcare settings and organizations.

It is important to identify individuals who are prone to pressure injuries. I have a son with cerebral palsy. He is in a wheelchair and lacks movement without assistance. He receives a body check twice a day, but even with my constant supervision, an ulcer can creep up quickly. My son's feet had become swollen and hot. The doctor placed him on antibiotics, but his left foot continued to get worse. A few days later, I took a photo of my son's wound and showed it to the doctor. The doctor immediately contacted a wound care nurse and his ankle was diagnosed as a stage II pressure ulcer. The wound healed eventually. It took about 6 weeks. Be your family and/or friend's advocate.
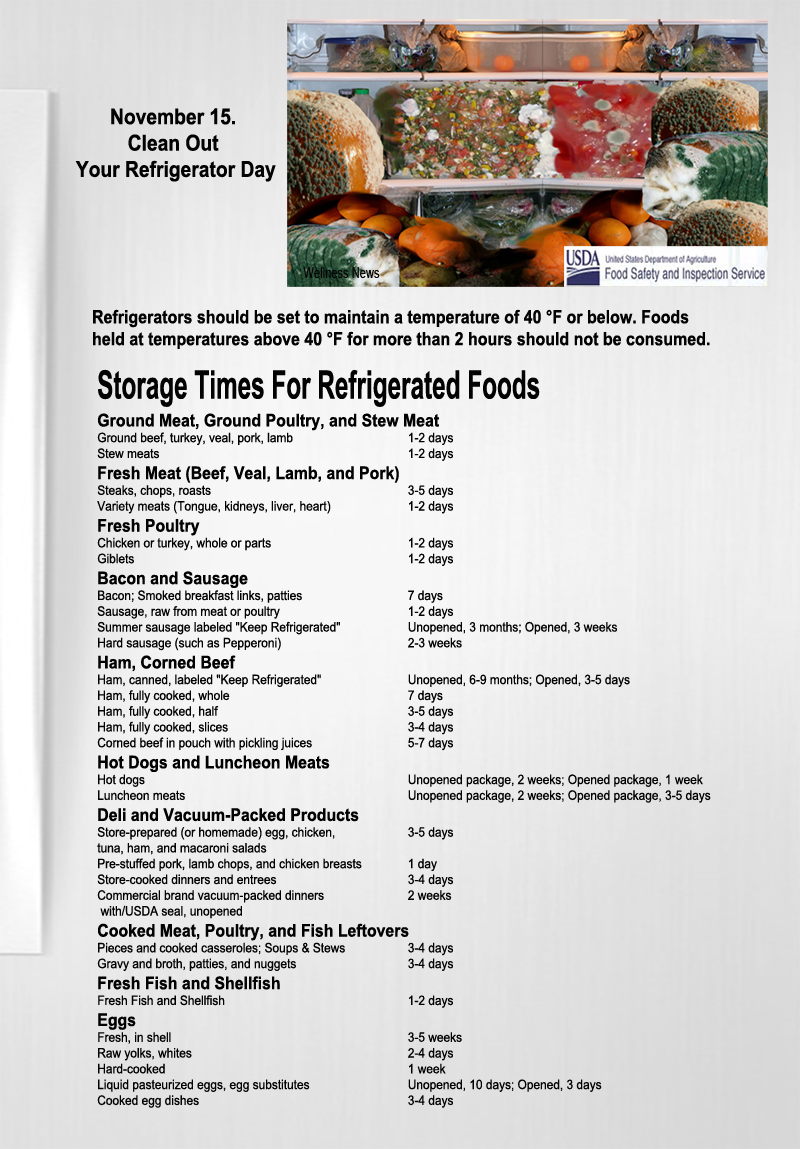
Skin Care
1. Inspect all of the skin upon admission as soon as possible (but within 8 hours).
2. Inspect the skin at least daily for signs of pressure injury, especially nonblanchable erythema.
3. Assess pressure points, such as the sacrum, coccyx, buttocks, heels, ischium, trochanters, elbows, and beneath medical devices.
4. When inspecting darkly pigmented skin, look for changes in skin tone, skin temperature, and tissue consistency compared to adjacent skin. Moistening the skin assists in identifying changes in color.
5. Cleanse the skin promptly after episodes of incontinence.
6. Use skin cleansers that are pH balanced for the skin.
7. Use skin moisturizers daily on dry skin.
8. Avoid positioning an individual on an area of erythema or pressure injury.
Nutrition
1. Consider hospitalized individuals to be at risk for undernutrition and malnutrition from their illness or being NPO for diagnostic testing.
2. Use a valid and reliable screening tool to determine the risk of malnutrition, such as the Mini Nutritional Assessment.
3. Refer all individuals at risk for pressure injury from malnutrition to a registered dietitian/nutritionist.
4. Assist the individual at mealtimes to increase oral intake.
5. Encourage all individuals at risk for pressure injury to consume adequate fluids and a balanced diet.
6. Assess weight changes over time.
7. Assess the adequacy of oral, enteral and parenteral intake.
8. Provide nutritional supplements between meals and with oral medications, unless contraindicated.
Repositioning and Mobilization
1. Turn and reposition all individuals at risk for pressure injury, unless contraindicated due to medical conditions or medical treatments.
2. Choose a frequency for turning based on the support surface in use, the tolerance of skin for pressure and the individual’s preferences.
3. Consider lengthening the turning schedule during the night to allow for uninterrupted sleep.
4. Turn the individual into a 30-degree side-lying position, and use your hand to determine if the sacrum is off the bed
5. Avoid positioning the individual on body areas with pressure injury.
6. Ensure that the heels are free from the bed.
7. Consider the level of immobility, exposure to shear, skin moisture, perfusion, body size, and weight of the individual when choosing a support surface.
8. Continue to reposition an individual when placed on any support surface.
9. Use a breathable incontinence pad when using microclimate management surfaces.
10. Use a pressure-redistributing chair cushion for individuals sitting in chairs or wheelchairs.
11. Reposition weak or immobile individuals in chairs hourly.
12. If the individual cannot be moved or is positioned with the head of the bed elevated over 30°, place a polyurethane foam dressing on the sacrum.
13. Use heel offloading devices or polyurethane foam dressings on individuals at high-risk for heel ulcers
14, Place thin foam or breathable dressings under medical devices.
Education
1. Teach the individual and family about risk for pressure injury
2. Engage individual and family in risk reduction interventions
Staging Pressure Injury
A pressure injury is localized damage to the skin and underlying soft tissue usually over a bony prominence or related to a medical or other devices. The injury can present as intact skin or an open ulcer and may be painful. The injury occurs as a result of intense and/or prolonged pressure or pressure in combination with shear. The tolerance of soft tissue for pressure and shear may also be affected by microclimate, nutrition, perfusion, co-morbidities and condition of the soft tissue.
Stage 1 Pressure Injury: Non-blanchable erythema of intact skin. Intact skin with a localized area of non-blanchable erythema, which may appear differently in darkly pigmented skin. The presence of blanchable erythema or changes in sensation, temperature, or firmness may precede visual changes. Color changes do not include purple or maroon discoloration; these may indicate deep tissue pressure injury.
Stage 2 Pressure Injury: Partial-thickness skin loss with exposed dermis. Partial-thickness loss of skin with exposed dermis. The wound bed is viable, pink or red, moist, and may also present as an intact or ruptured serum-filled blister. Adipose (fat) is not visible and deeper tissues are not visible. Granulation tissue, slough and eschar are not present. These injuries commonly result from adverse microclimate and shear in the skin over the pelvis and shear in the heel. This stage should not be used to describe moisture associated skin damage (MASD) including incontinence associated dermatitis (IAD), intertriginous dermatitis (ITD), medical adhesive related skin injury (MARSI), or traumatic wounds (skin tears, burns, abrasions).
Stage 3 Pressure Injury: Full-thickness skin loss. Full-thickness loss of skin, in which adipose (fat) is visible in the ulcer and granulation tissue and epibole (rolled wound edges) are often present. Slough and/or eschar may be visible. The depth of tissue damage varies by anatomical location; areas of significant adiposity can develop deep wounds. Undermining and tunneling may occur. Fascia, muscle, tendon, ligament, cartilage and/or bone are not exposed. If slough or eschar obscures the extent of tissue loss this is an Unstageable Pressure Injury.
Stage 4 Pressure Injury: Full-thickness skin and tissue loss. Full-thickness skin and tissue loss with exposed or directly palpable fascia, muscle, tendon, ligament, cartilage or bone in the ulcer. Slough and/or eschar may be visible. Epibole (rolled edges), undermining and/or tunneling often occur. Depth varies by anatomical location. If slough or eschar obscures the extent of tissue loss this is an Unstageable Pressure Injury.
Unstageable Pressure Injury: Obscured full-thickness skin and tissue loss. Full-thickness skin and tissue loss in which the extent of tissue damage within the ulcer cannot be confirmed because it is obscured by slough or eschar. If slough or eschar is removed, a Stage 3 or Stage 4 pressure injury will be revealed. Stable eschar (i.e. dry, adherent, intact without erythema or fluctuance) on the heel or ischemic limb should not be softened or removed.
Deep Tissue Pressure Injury: Persistent non-blanchable deep red, maroon or purple discoloration. Intact or non-intact skin with a localized area of persistent non-blanchable deep red, maroon, purple discoloration or epidermal separation revealing a dark wound bed or blood-filled blister. Pain and temperature changes often precede skin color changes. Discoloration may appear differently in darkly pigmented skin. This injury results from intense and/or prolonged pressure and shear forces at the bone-muscle interface. The wound may evolve rapidly to reveal the actual extent of tissue injury, or may resolve without tissue loss. If necrotic tissue, subcutaneous tissue, granulation tissue, fascia, muscle, or other underlying structures are visible, this indicates a full-thickness pressure injury (Unstageable, Stage 3, or Stage 4).